Carlo Perfetti Neurocognitive Rehabilitation
The approach according to Carlo Perfetti for post-stroke recovery, based on the activation of cognitive processes for motor reorganization.
What is Neurocognitive Rehabilitation?
It is the rehabilitation approach that originated in Italy in the late 1960s from the studies of the Italian physician Carlo Perfetti. For this reason, it is more widely known as the Perfetti Method and Cognitive Therapeutic Exercise (C.T.E.).
How did the Perfetti Method begin?
Carlo Perfetti specialized in the Clinic of Mental and Nervous Diseases. In the late 1960s, he began to take an interest in rehabilitation, specifically in the rehabilitation of patients with stroke, infantile cerebral palsy, and spasticity. He studied with interest the neuromotor physiotherapy methods popular at that time, such as the Vojta, Kabat, and finally Bobath methods. The latter was considered by the Tuscan physician to be the most interesting approach available, but at the same time he began to become passionate about a problem that had until then remained unresolved and was considered insurmountable: the recovery of the hand in the hemiplegic patient.
From the development of this problem and from the historical, social, cultural, and scientific influences of that period, he began to create a theory of rehabilitation that also considered the patient’s cognitive processes, and not only the ability to contract muscle fibers and activate reflex patterns. If stroke affects the patient’s brain, then brain functions must be considered during exercise; this premise broadly summarizes the therapeutic identity of cognitive treatments.
How does the Perfetti Method work?
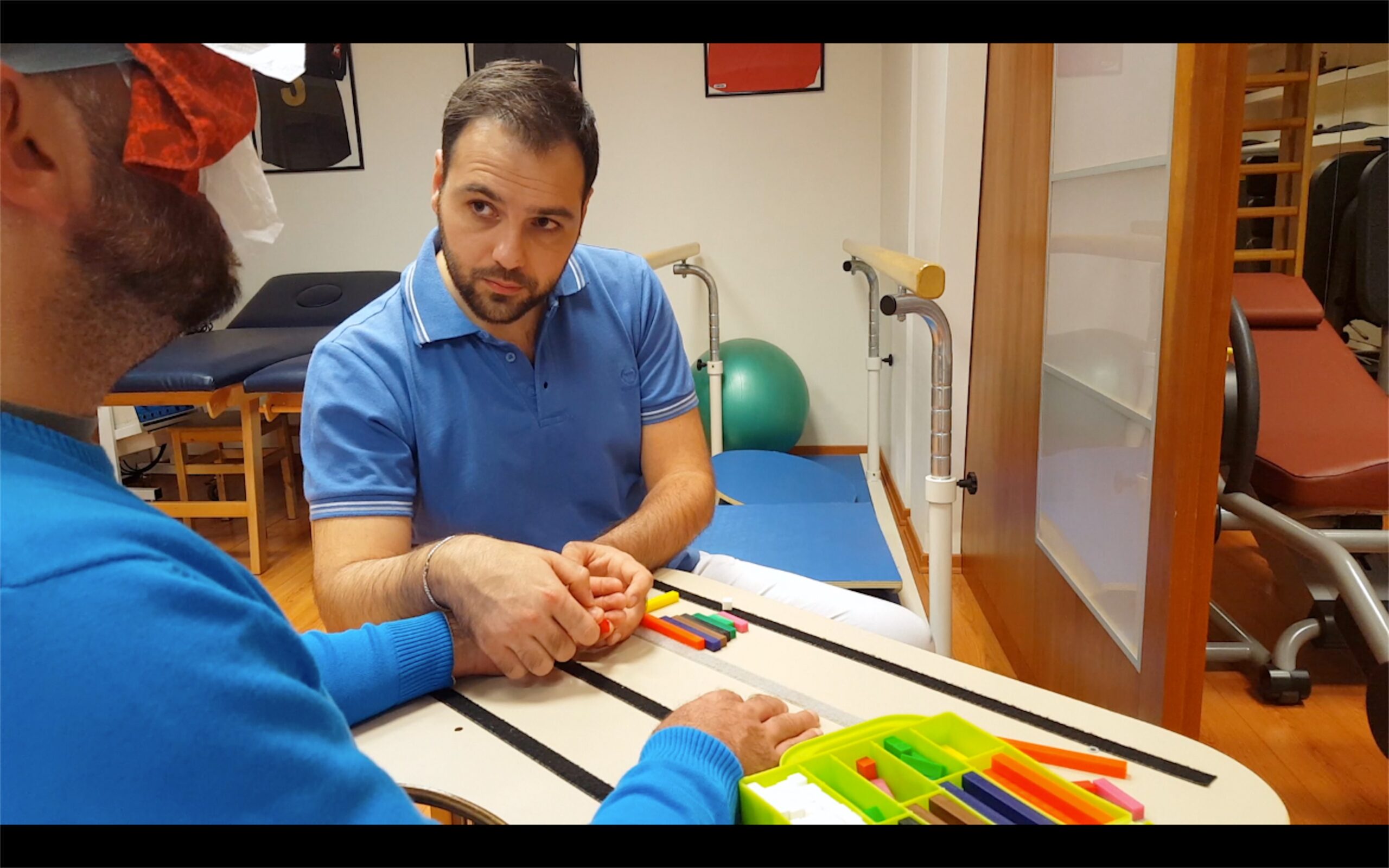
To get to the heart of the neurocognitive method, we believe it is useful to show an example of an exercise so that its characteristics and differences from the activities we are used to seeing with patients with neurological conditions, and specifically with the consequences of stroke, become immediately clear. As we will see later, however, this is a working method that can be applied to all conditions requiring physiotherapy, not only to those who have suffered a stroke.
Before watching the video, a few clarifications are necessary: the exercise is a personalized experience that the rehabilitation therapist builds according to the needs of the individual patient. The video we will show is only part of a strategy to begin orienting ourselves within the principles of neurocognitive rehabilitation, to provide an initial understanding. We also invite you to try it at home, even with your family, to get a clearer idea, while keeping in mind that every activity must be created “tailor-made” for the person… WITH the person.
Let us discuss the characteristics and differences…
I have often visited clinics where I had been invited to teach training courses. The directors proudly showed me their cutting-edge gyms, equipped with the best equipment and technical-computer systems, but almost all of them had one thing in common: a series of treatment tables facing one another, where patients were lying down while therapists performed various maneuvers and mobilizations on them. These were sometimes convivial spaces where therapists spoke among themselves or with patients about personal or current topics. In this setting, the environment and the manual practices of the therapists placed patients in a passive position without involving attention toward the body. In the video just shown, however, this is one of the specific features of the neurocognitive exercise: the patient would not have been able to recognize the circle without using attention.

Why can therapeutic exercise after a stroke not do without attention?
We must always remember that a stroke affects the brain, not the muscles. Even though the patient has maintained their intelligence, remains the same bright person, and has not lost their abilities to the point of being able to return to work, this does not mean that they have not experienced changes in attention toward the body. Many readers who are patients or family members will remember the first weeks or months when, especially in patients with left hemiparesis, there was a certain difficulty in looking at and paying attention to the side of the lesion. This syndrome is called neglect, and it is not a problem of vision, but of attention toward the information coming from the side of the body affected by the paresis. Even if, in the following months and also with the help of family members, the patient has learned to make an effort to look toward the paralyzed side, some attention deficits toward the body often remain, and these represent an obstacle to the recovery of motor ability. Patients with right hemiplegia also suffer from disorders of attention toward the body and movement; some readers may have heard the term apraxia from a professional. In this clinical picture as well, the patient has difficulty directing attention toward the body. For patients who have never been associated with an attention disorder such as neglect or apraxia, another fundamental aspect must be considered: if the damage occurred in the brain, and it is the brain that needs to be reactivated to create new connections, having a part of the body moved, or moving it without directing attention in a specific way, may not lead to the desired goals and results.
Among the other differences, we find the act of closing the eyes. In the early stages of treatment, this helps the patient give priority to sensations coming from the body rather than from sight. In the neurocognitive exercise shown in the video, memory also plays an important role. I am aware that when I mention memory as an important cognitive element for improvement, the patient feels that they have not lost it; in fact, on many occasions they report having an even more trained memory and remembering many more things after the stroke. Here I must clarify that the memory that may have been impaired is not the one linked to the patient’s personal history or computer passwords. I am referring to the memory closely related to bodily sensations, the memory of the body in action; this is what may have been altered after a stroke and needs to be reactivated.
The use of perception is clear in the video, and the reason why it is important for physiotherapy to consider perception is that movement cannot be studied while excluding what we are able to perceive through our interaction with objects and the environment. These are precisely the pieces of information that guide movement, which in turn aims to collect increasingly precise information. In this case as well, the patient may report not having suffered any perceptual deficit, remembering the neurologist’s examinations in the hospital, when during evaluation the doctor pressed the tip of a pen on the skin or sometimes touched a part of the body with a finger, asking whether the patient could perceive it. However, the perception we need to perform movement goes far beyond simply feeling whether or not there is contact on the skin. It also requires the ability to recognize the exact position in space of all our body segments; this ability is called kinesthesia.
Interestingly, the therapist did not ask the patient to participate in the movement by voluntarily lifting or opening the arm, but asked the patient to let themselves be guided. We are therefore faced with the absence of a request for visible muscle contractions. I feel it is important to add the adjective “visible,” because in an exercise where the patient is asked to let themselves be guided and therefore to adapt muscle tone, which as we know after a stroke often appears hypertonic and spastic, this does not mean that the patient is not participating in the movement or that the exercise is passive. In fact, in order to let themselves be guided, the stroke patient must control muscle tone and learn to reduce tension, which represents an obvious obstacle to recovery in terms of quality. I understand that the patient may believe that in order to recover they must make efforts and commit themselves to moving, but unfortunately the reality of the consequences of brain injury is different. In order to learn to move, effort may even be counterproductive, increasing the spasticity that the patient wants to resolve.
We also notice differences in the therapist’s language compared with traditional physiotherapy. Here, the professional does not use language to give orders that the patient must satisfy with a motor response. Rather, it is language that supports the resolution of a problem, which is another major protagonist of Perfetti’s neurocognitive exercise, because it is capable of activating all the cognitive processes necessary for its solution. The stimulation of cognitive processes to fragment the body affects the development of learning and motor skills. This is not a purely mental exercise, as might occur during a neuropsychological evaluation, but a true motor and cognitive rehabilitation exercise at the same time.
Who is the Perfetti Method suitable for?
In these twenty years of work as a neurocognitive rehabilitation therapist, I have had the opportunity to listen to many patients who had often been given incorrect information about the method: some claimed that the method was not suitable for patients without cognitive deficits, while others, on the contrary, believed it was not suitable for those who did have cognitive problems. As we discussed in the previous paragraphs, having cognitive disorders does not necessarily mean having dementia or having lost one’s mind. We must consider cognitive functions as functions of the brain, just as we attribute respiratory functions to the lungs and circulatory functions to the heart. It is clear that an injury to the lungs or heart, if not fatal, will have more or less evident repercussions depending on its severity. The same occurs in the brain when it suffers a stroke, and therefore a lesion caused by ischemia or hemorrhage.
As a professional, when I refer to a patient with cognitive disorders, I am referring to all stroke patients who may have some sensory deficits, some difficulty considering parts of the body, remembering certain aspects of movement, building a prediction of the complete action, or learning new movements. All these elements lead to the absence or alteration of movement, but they do not coincide with the patient’s intelligence, which I firmly repeat I am certain has not been altered, and which may also allow a complete return to work and social life. As for the alleged unsuitability of the method for individuals with cognitive disorders, unfortunately this statement is made by those who are unfamiliar with the neurocognitive approach and probably, in broader terms, with rehabilitation itself. Professionally and ethically, it is clear that a patient with cognitive disorders needs therapy that helps activate and reorganize them.
The method is therefore suitable for all patients who, after suffering a stroke, need to recover and improve movement.
For which conditions is the Perfetti Method suitable?
Here too, a clarification is necessary. I often refer to patients with hemiplegia, meaning those who have suffered a stroke, and our Stroke Therapy Revolution rehabilitation programs are also exclusively for people with the consequences of stroke and not other diseases. However, this does not mean that the method cannot be applied to other neurological, orthopedic, or rheumatological conditions.
Prof. Carlo Perfetti began his studies with brain injuries, and most of his research involved stroke. This was a specific passion of his, which he passed on to us as students. However, among Perfetti’s students there are also those who specialized in developmental age disorders, parkinsonian syndromes, multiple sclerosis, and orthopedic syndromes, as well as cases of neuropathic pain caused by stroke itself or phantom limb pain after amputation. We also offer our students attending courses at our Neurocognitive Academy a training plan especially focused on stroke rehabilitation, but all enrolled professionals are aware that each of them will apply neurocognitive theory within their own area of interest.
Perfetti Method, Neurocognitive Rehabilitation, or Cognitive Therapeutic Exercise?
In essence, there is no difference; these are simply the names by which the approach developed by Carlo Perfetti is known. The reason for the change in names is that names define things, and if things change over time, names should adapt as well. This is why, over time, the first name, “Progressive Sequential Control,” became “Cognitive Therapeutic Exercise,” because neurocognitive theory cannot be fixed and static, since neuroscience offers new contributions every day, shaping and refining it.
“Perfetti Method” was the name the public gave to this approach, but the Professor himself always viewed this term with caution because it was not suitable for an approach that moves away from a technique made of predefined patterns and maneuvers. Later, the term Neurocognitive Rehabilitation was adopted, highlighting the interest in the body (neuro) and in mental processes (cognitive). Once again, the reference to Perfetti is spontaneously associated with this term, both to distinguish it from neurocognitive rehabilitation in the psychological field and to pay proper tribute to its creator.
Finally, a more recent proposal was to call it “Comparison between actions,” a term capable of explaining the professor’s latest contributions regarding the structure of the exercise. Personally, I feel the need to respect Prof. Perfetti’s rigor, but also to make the subject understandable to the public. For this reason, I prefer to use the term Cognitive Rehabilitation according to Perfetti, but at times, as in this article, I use “Perfetti Method” to help the reader frame the topic.
Author
Valerio Sarmati
Graduate in Physiotherapy and Rehabilitation Health Professions, specialized in Neurocognitive Rehabilitation of post-stroke patients.
Lecturer in neurotraumatological rehabilitation in the physiotherapy degree program, and in Neurocognitive Rehabilitation in the neurorehabilitation master’s program at the University of Rome La Sapienza.
Contact
Some Useful Resources